Tony M. Woodward, DVM, Diplomate AVDC
Animal Dental Care, Colorado Springs, Colorado
Current standards of care in veterinary medicine dictate an adequate level of pain control
for our patients. Effective pain control employs a proactive, multi-mode approach that starts with pre-operative medications, includes the anesthetic protocol selected, and continues into the postoperative period. Local (regional) anesthesia plays an important part in the pain control of oral surgical patients. These techniques are used for a number of common oral procedures, including extractions, periodontal flap surgery, treatment of traumatic injuries of the oral cavity, tumor removal, palatal surgery, and root canal therapy.
Local anesthetics exert their effect by preventing cell membrane depolarization of the
afferent neuron. The permeability of the neuronal cell membrane to sodium ions is decreased, which prevents the propagation of the nerve impulse beyond the area of the block. Local anesthetics also act as vasodilators, which can increase bleeding and effectively reduce efficacy, due to the product being carried away by increased blood flow. The addition of some type of vasoconstrictor, such as epinephrine, can significantly extend the time of action and help counteract the tendency toward increased bleeding.
The use of local anesthesia provides several benefits for the patient. Local anesthesia
allows a decreased plane of general anesthesia required to complete a procedure. Decreasing the level of general anesthetic agents improves blood pressure intra-operatively, and contributes toward more rapid anesthetic recovery. Additionally, local anesthesia can provide analgesia for several hours in the immediate perioperative period. Finally, the use of local anesthesia represents another mode of pain relief that work synergistically with other modalities such as narcotics, alpha-2 agonists and NSAIDS.
Materials required for local anesthesia are simple and inexpensive. Several agents are
commonly used for nerve blocks, and they vary as to their time of onset and duration of action as seen below. The selection of an agent with a combined vasoconstrictor (epinephrine) will tend to make the block last toward the longer end of the ranges noted below. The use of epinephrine is contraindicated in patients with uncontrolled hyperthyroidism, cardiac dysrythmias, and asthma. Consider using bupivacaine with epinephrine whenever possible, and use either bupivacaine or mepivacaine without epinephrine when epinephrine is contraindicated.

The anesthetic agents are available in multiple dose vials or in 1.8 ml cartridges, which
are placed in a dental aspirating syringe. The dental syringes work well for aspirating with one hand, but the cartridges for these syringes are significantly more expensive than the multiple dose vials. Available needle sizes for the aspirating syringes are 25, 27, and 30 gauge in either 1 or 1 3/8 inch lengths. Alternatively plain syringes and luer-type needles can be used when employing the multiple dose vials. I prefer to use plain 1 or 3 cc syringes and 25-gauge 1 1/2inch needles for most nerve blocks. With feline patients, a 27-gauge needle can assist entry into smaller foramina.
Complications of local anesthesia may include dysrythmia secondary to intravascular
administration, bronchospasm (if epinephrine was utilized), neuropathy secondary to trauma, and bleeding/hematoma. When administering the inferior alveolar (mandibular) nerve block, it is possible to inadvertently block the lingual nerve, which innervates the tongue. This may lead to self-mutilation in the patient upon recovery. Due to the low volumes of agent used in small patients, it can be easy to exceed a safe total body dose of the anesthetic agent, leading to cardiorespiratory depression and possible death. Although each of the agents utilized has their own safe doses, an easily rule of thumb is to keep your total body dose under 2 mg/kg BW, regardless of the agent being utilized. In small patients, it may be safest to draw up the total calculated body dose at the beginning of the procedure. When the contents of this syringe are gone, no additional agent should be drawn up. In general, nerve blocks in the feline require 0.1 to 0.3 ml, and those in canines require 0.1 to 0.5 ml per site. For all nerve blocks, you should aspirate prior to injection to decrease the chances of intravascular administration. The following four blocks are
the ones used most commonly in canine and feline patients.
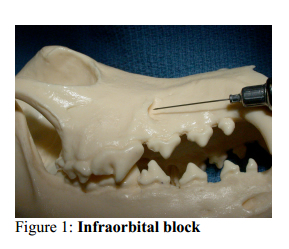
Infraorbital Block (Figure 1)
Anatomy: The infraorbital nerves innervate the dental structures in each side of the
maxilla and incisive bone. The infraorbital nerve is the major terminal division of the maxillary branch of the trigeminal nerve. The caudal superior alveolar nerve branches off the infraorbital nerve as it enters the infraorbital canal and supplies innervation to the fourth premolar and both molars. The middle superior alveolar nerve branches off the infraorbital nerve in the middle of the infraorbital canal and supplies the first through third premolars. The cranial superior alveolar nerve branches off the infraorbital nerve just before it leaves the infraorbital canal and supplies innervation to the canine tooth and incisors on that side.
Area blocked: Depending on the level at which the block is placed, you can effectively
block the teeth, bone, and buccal soft tissue from either the canine tooth forward, from the third premolar forward, or the entire maxillary arcade.
Technique: The infraorbital foramen is easily palpated above the distal (caudal) root of
the third upper premolar. Start the needle through the oral mucosa in a caudal direction, and insert the needle into the infraorbital canal an appropriate distance for the area requiring blockage. Placement of the agent just inside the infraorbital canal will block the ipsilateral canine tooth and incisors. Placement of the block in the central area of the infraorbital canal will block from the third premolar forward, and placement of the block at the caudal extent of the infraorbital canal (next to the maxillary foramen) will block the entire arcade, as well as the hard and soft palatal structures. The caudal extent of the infraorbital canal is located at the level of the medial canthus of the eye, which serves as a guide for maximum needle advancement. In all cases, firm digital pressure over the infraorbital foramen during injection and for 60 seconds afterward will encourage diffusion of the agent in a posterior direction, improving the likelihood of an effective block. The same technique is used in feline patients and brachycephalic dogs, being cautious to avoid inserting the needle beyond the medial canthus, as the infraorbital canal is rather short compared to normocephalic and dolichocephalic dogs.

Maxillary block (Figures 2 and 3)
Anatomy: Some authors prefer the maxillary block when trying to achieve anesthesia of
an entire maxillary quadrant. The disadvantage of this technique is that it involves blind
placement of the anesthetic agent into the retrobulbar space, which is occupied by a number of vital structures. The advantage of this technique is that it may provide for improved anesthesia of the last premolar and molars.
Area blocked: All dental, bone, and soft tissues of the entire maxillary quadrant,
including the soft and hard palatal structures on that side.
Technique: Palpate the ventral aspect of the zygomatic arch where it joins the maxilla.
The needle should be directed dorsally, adjacent to the bone, advancing it to the approximate level of the root tips of the last molar. In the cat, this area is best reached through the infraorbital canal, using the infraorbital block previously described

Major Palatine Block (Figure 4)
Anatomy: The major palatine nerve arises from the major palatine foramen and supplies
innervation to the hard and soft palatal structures. The major palatine foramina in the dog are located on a transverse line connecting the center of the upper fourth premolars. The nervescourse cranially, approximately halfway between the midline of the palate and the dental arcade. In the cat, the major palatal foramina are located slightly cranial to the position in the dog.
Area blocked: Bone and soft tissue of the hard and soft palate and the palatal aspect of the gingiva surrounding the maxillary arcade.
Technique: Place the block just caudal to the area desired to be blocked. Imagine the line
halfway between the midline and arcade, advance the needle to the palate, and place the block. An obvious bleb will be seen, confirming the placement of the block. The technique is the same in the cat, with the major palatine foramina being located on a line connecting the palatal cusps of the upper fourth premolars (Figure 5).

Mental (Middle Mental) Block (Figure 6)
Anatomy: The middle mental nerve exits the middle mental foramen, which in the dog is
located on the lateral aspect of the mandible, below the mesial (cranial) root of the lower second premolar. The foramen is slightly closer to the ventral cortex than the alveolar bony ridge. Typically, the foramen is located on the caudal edge of the labial frenulum. In the cat, the foramen is located between the third premolar (which is the most rostral premolar in the cat) and the canine tooth, halfway down the lateral aspect of the mandible. In cats this may also be visualized as being located lateral to the apex of the lower canine tooth.
Area blocked: If the block is placed outside the foramen, only soft tissues around the
ipsilateral canine teeth and incisors are affected. If the block is placed inside the mental foramen and digital pressure is maintained to force the agent to diffuse caudally into the mandibular canal, the dental structures and bone will also be affected. In the cat, it is difficult to place the block inside the foramen due to its small size.
Technique: Place the needle just cranial to the location of the foramen, which can be
readily palpated in larger patients. Direct the needle in a posterior fashion, and if possible direct the needle into the foramen as far as possible. If you cannot place the block into the foramen, simply place the block around the outside of the foramen.Inferior Alveolar (Mandibular) Block (Figure 7)
Anatomy: The mandibular nerve enters the mandible on the medial side and provides
sensation to the teeth and bone on the ipsilateral side. The foramen is located approximately halfway between the angular process of the mandible and the cranial aspect of the coronoid process of the mandible caudal to the last mandibular molar. Before entering the mandibular foramen, the lingual nerve braches off, supplying the tongue. This is clinically significant, as this block may inadvertently result in lingual anesthesia and secondary self-mutilation of the tongue.
Area blocked: All dental and bony structures of the ipsilateral mandible.
Technique: This block may be placed in either an intra-oral or extra-oral fashion. If the
extra-oral technique is used, a small area on the ventral mandible just rostral to the angular process is clipped and prepped. The ventral surface of the mandible is palpated for the small notch present just cranial to the angular process. In smaller dogs and cats, it may not be possible to palpate this notch. The needle is introduced through the skin below this notch, and is walked up the medial aspect of the mandible approximately halfway up the mandible. For the intra-oral technique, the thumb is placed on the cranio-ventral aspect of the coronoid process of the mandible, and the forefinger of the same hand is placed on the angular process. An imaginary line is drawn between these two fixed points, and the needle is introduced on the medial aspect of the mandible and advanced along this line, approximately half the distance to the angular process. Regardless of which technique is used, in many patients it is possible to palpate the mandibular nerve and foramen intra-orally to help confirm the placement of the needle prior to injection. This block is done in a similar fashion in the cat.

Splash Block
One other block that may be used in oral surgery is the “splash block.” A splash block is
simply either injected into tissues in the surgical site or placed into a closed space where it may diffuse. Examples would include placement of the anesthetic agent into a sutured extraction site, where the agent is allowed to diffuse into the tissues of the extraction site.Beckman B, Legendre L: Regional nerve blocks for oral surgery in companion animals.
Compend Cont Ed Pract 2002; 24: 439
Lantz G: Regional anesthesia for dentistry and oral surgery. J Vet Dent 20:181-186, 2003.
Tranquilli W, Grimm K, Lamont L: Pain management for the small animal practitioner. Jackson, Wyo, Teton New Media, 2000, pp 48-52.